Oxygen and Your Ears
by Jeffrey Bozanic
Immersed, Winter 2003, (7:4) pp. 42-46
Richard and John arrived on Andros Island in the Bahamas at noon, and by five o'clock were in the water on their first deep dive of their weeklong vacation. Their dive was on the wreck of the Holly, located at a depth of 245 fsw (75 msw), with their 25-minute bottom time necessitating two hours of decompression. Richard was using a mixed gas closed circuit rebreather (CCR), while John was diving open circuit air (twins), and carrying cylinders containing EAN36 and oxygen for decompression. Conditions were generally good, with 82oF (28C) water, no current, 165-foot (50m) visibility, and a 1-2 foot (0.5m) swell running. The dive went off without a hitch, and they exited the water at 7:30 p.m. An hour later, they were both in bed, tired from their seven-hour plane rides and the excitement of the first dive. The next morning, both Richard and John awoke to find their ears very sore and filled with fluid.


What happened? Did they pick up an infection on the plane ride? Was there a pathogen or nasty chemical in the water? Some strange decompression hit? Maybe a fungus in the hotel room? Was it from the swells that forced them to equalize every few seconds during the decompression stops, even though they felt fine during the dive? It seemed unlikely to be an equipment related problem of some type, as one used a CCR and the other twin open circuit cylinders. All they knew was they felt fine the day before, and now the doctor had recommended not diving for a week, giving the fluid he could see behind their tympanic membranes time to drain and their ears time to return to normal. So much for their diving vacation!
In actuality, both of them had squeezes. Squeezes?! How could they have an ear squeeze if they had no problems during the dive?! During our initial dive training we were taught that if we failed to equalize as we descended, then a pressure imbalance could create a painful condition known as a squeeze. We were also taught that in some circumstances, during ascent if the Eustachian tube was blocked we could also get a squeeze, called a reverse block. Either way, once we returned to the surface, and dive was over, the threat of ear squeeze was eliminated as well. This is not true with some forms of technical diving.
Susceptibility to oxygen ear squeezes will begin when this diver exits the water.
TECHNICAL TIP: Divers using rebreathers should also take into consideration the risk of middle ear oxygen absorption syndrome. Periodic manual equalization after surfacing can prevent the syndrome and should be a regular post-diving procedure.


Divers learn that upon returning to the surface at the end of the dive, the threat of ear squeeze is eliminated as well. This is not true with some forms of technical diving.
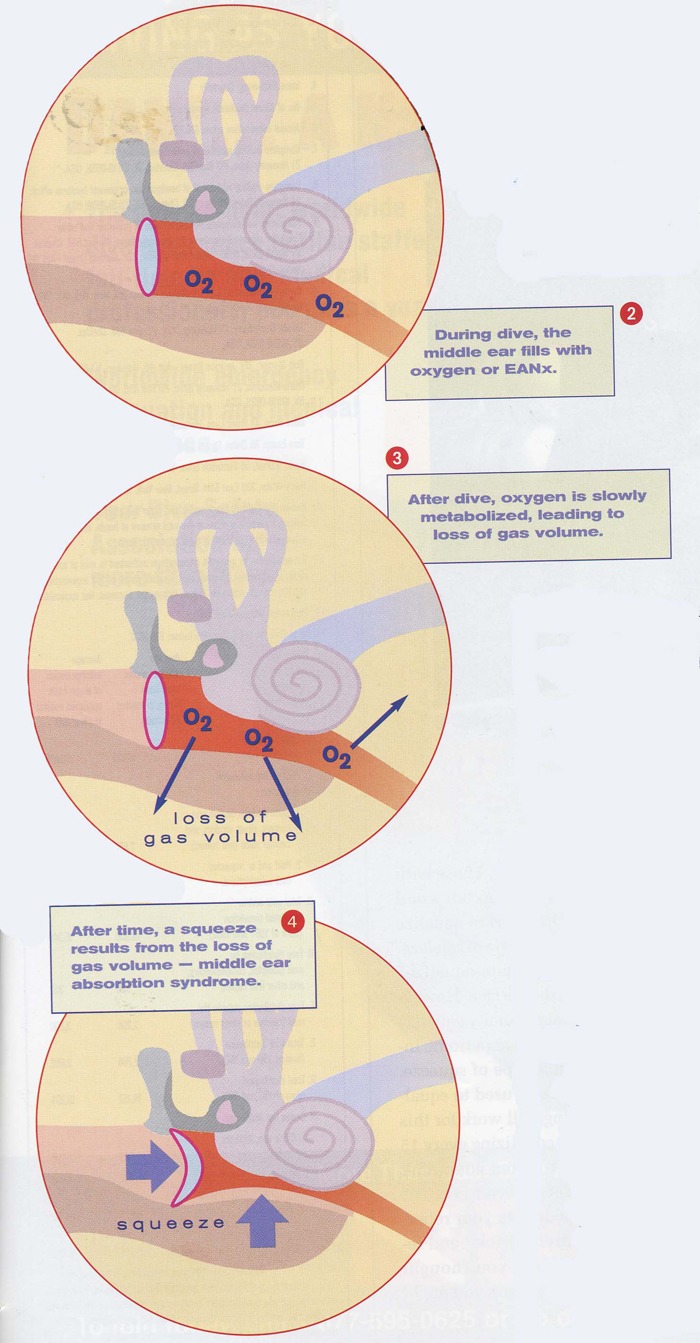
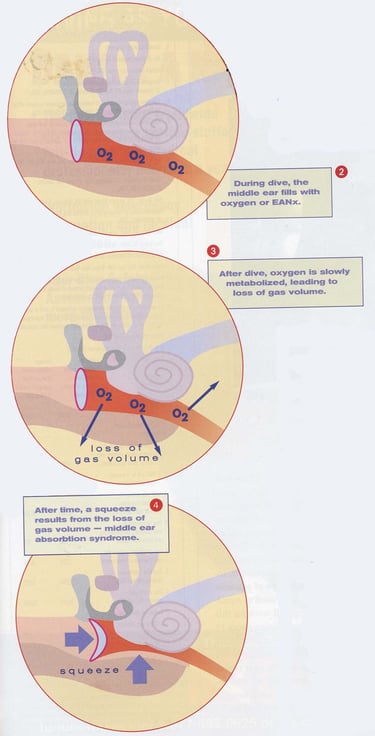
In open circuit diving while using air, divers descend and equalize with air. The gas filling their middle ears is the same as the gas they are breathing on the surface. In technical diving, this may not be true. For example, in our story above, Richard was using a rebreather. Typically, in mixed gas CCRs, the oxygen fraction (percentage of oxygen in the breathing mix) is very high at the beginning of the dive, typically 0.7 (70%) or higher. Thus, the middle ear is filled with gas containing a high concentration of oxygen.
During the dive, this presents no problem, as the diver equalizes whenever a pressure imbalance is felt. However, upon reaching the surface, divers no longer consider the need to equalize, as they have reached a stable pressure. But their middle ears may still be filled with an oxygen-rich gas. Slowly, over time, the oxygen in the middle ear may be metabolized (used) by the tissues surrounding the area. The volume of gas slowly decreases, resulting in a net pressure imbalance between the outer and middle ear. This can result in a squeeze, identical in effect to that experienced by descending without equalizing.
This type of squeeze is known as middle ear oxygen absorption syndrome, or "O2 ear." It is also seen in military aviators as well, who commonly use oxygen during high altitude operations and experience the squeeze some time after landing. Because onset is so gradual, an individual may not notice the pressure imbalance until noticeable damage has occurred. This is especially true if one goes to sleep soon after the causative event.
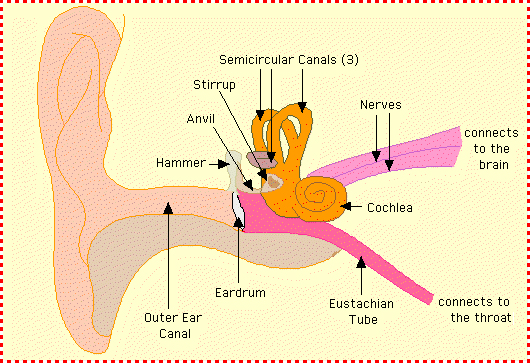
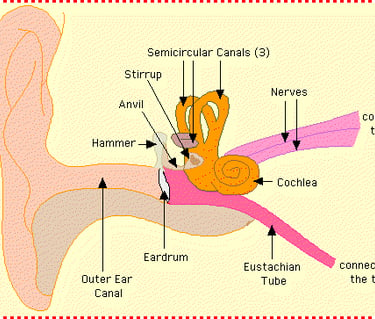
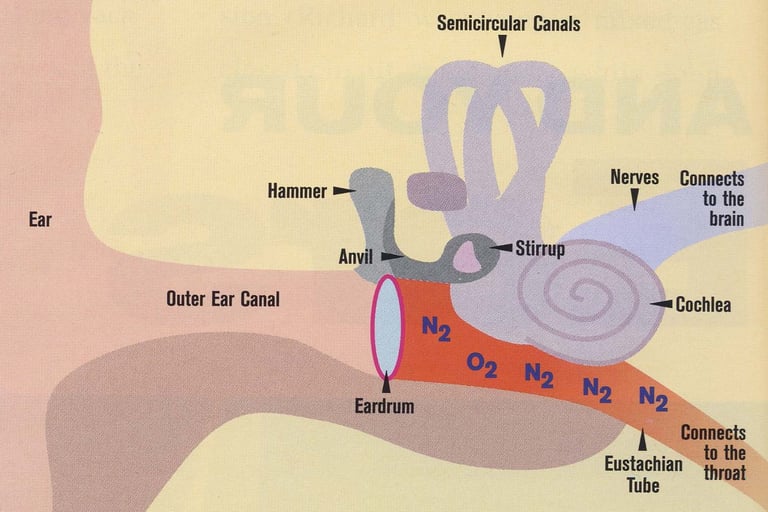
Normal middle ear physiology
Middle ear prior to diving
Middle ear oxygen absorption occurring
Are you in the risk group for this potential health problem? You may be if you use: (1) an oxygen rebreather, (2) a semi-closed rebreather with high-fraction nitrox supply gas, (3) a mixed gas CCR, (4) any high fraction nitrox during open circuit diving. The risk is generally less for open circuit divers, as descent (and pressure equalization) usually occurs on air or whatever bottom mix is being utilized. The use of oxygen or high fraction nitrox mixes is generally constrained to use at decompression stops, not during descents. However, if any event forces you to equalize often while at decompression (for example swells passing overhead, or depth drift during the stop), then you may also be at risk. This is what happened to John in our example above, who filled his middle ear spaces with oxygen while equalizing every time a swell passed overhead during the final 60-minute deco stop.
Not all fliers or divers will experience this problem, only those who routinely have to make some effort to equalize. Those with "sewer pipes" for Eustachian tubes and have to make no effort to equalize will not experience this type of squeeze, as they will generally "auto-equalize" even after reaching the surface. However, the rest of us must manually equalize after reaching the surface at periodic intervals to prevent this type of squeeze. Any maneuver that you typically use to equalize while descending will work for this purpose. Generally, equalizing every 15-30 minutes for 2-4 hours after the dive will prevent the syndrome.
So add this procedure to your repertoire of technical diving tricks, and remember that just when you thought you were safe from squeezes, you might not be….
All content, images and text copright © Jeffrey Bozanic (except as noted). All rights reserved worldwide. No images or text may be copied, duplicated, modified, or redistributed in part of whole (except for printing for personal reference) without prior written consent from Jeffrey Bozanic.